What is a tongue tie?

“Tongue-tie”, or “ankyloglossia”, has been recognized for centuries. It is a remnant of tissue (a lingual frenulum) left over from when the tongue is formed from the floor of the mouth, that exists to varying degrees in a large percentage of the population. If you sweep your finger from one side to the other at the base of your own tongue, you may feel a “speed bump” or a wall of tissue in the center. This is your “lingual frenulum”. It is composed of a fold of the mucosa (the lining of your mouth) and sometimes there is also a fold of “fascia” – (white, stiff connective tissue like you encounter when eating a steak) that can be present underneath the mucosa. Often the front part of the frenulum is thinner mucosa, and the back part is thicker. Very occasionally there is also some muscle contained within the frenulum. We just recently learned the anatomy of a lingual frenulum: What is a tongue tie? Defining the anatomy of the in-situ lingual frenulum. - Abstract - Europe PMC We at MilkWorks know about the lingual frenulum because in some babies it can restrict the movement of the tongue needed to latch onto a breast comfortably and remove milk well.
What does the tongue need to do to breastfeed effectively and comfortably?
It needs to gently pull the breast into the mouth and maintain contact to create a seal while the back of the tongue drops to create suction, as seen in this video.
The type of lingual frenulum that attaches near the tip of the tongue has been recognized for centuries, and the procedure where it is divided is called a lingual frenotomy. This procedure was done routinely until around 1960 when it was decided this was not necessary, and most everyone stopped clipping “tongue-ties”. Because the vast majority of babies were bottle-fed formula at that time, they could get enough to eat despite having a lingual frenulum. But then research started to pile up in the 1970s about how breastfeeding is actually a very good idea, and parents started to want to do it in the 80s, but no one knew how to help them anymore. So lactation consultants (IBCLCs) appeared in the 80s and 90s, and noticed they saw a LOT of tongue-tied babies. A study was published in 2000 noting that tongue-tie was more common in the breastfeeding clinic than the general nursery population and clipping of newborns tongue-ties began. 2000 - Ankyloglossia Incidence and Associated Feeding Difficulties Messner A (Arch Otolaryngol Head Neck Surg). In this study, feeding difficulties were found in 25% of babies with a tongue-tie vs those without a tongue-tie = 4.8% (1041 babies total).
More studies were done about how clipping could help with babies’ ability to latch onto the breast, mom’s latch comfort, and baby’s ability to remove milk. So, more and more people started clipping them (usually with scissors).
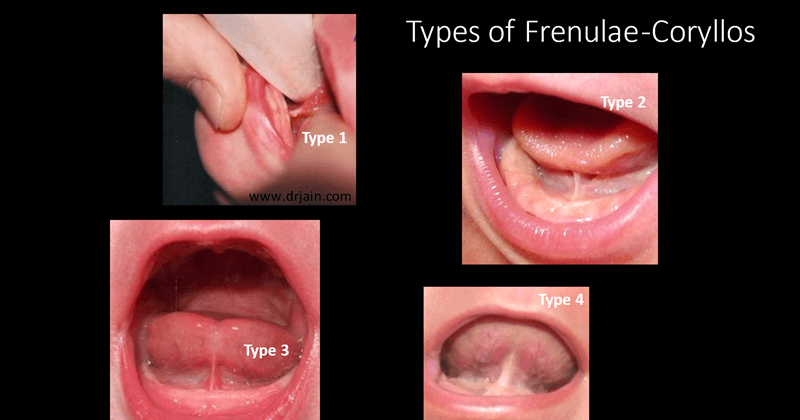
In addition, in 2013 a dentist in New York published some case reports (a case report describes one patient’s story) about using a laser to free up lip ties and started teaching other dentists how to use laser to eliminate tongue and lip “ties” around the country. Diagnosing and Understanding the Maxillary Lip-tie (Superior Labial, the Maxillary Labial Frenum) as it Relates to Breastfeeding. Lawrence A. Kotlow, DDS. A typing system was developed by a surgeon (Betty Coryllos, MD) in NYC to help describe where the tie attaches in the mouth; Type 1, 2, 3 and 4:
What is the procedure?
Also contributing to the confusion about lingual frenotomy is the fact that WE DO NOT HAVE AN ACCEPTED DEFINITION OF WHAT THE PROCEDURE ENTAILS!!! That’s right. In our community, there are Hospitalists, Pediatricians, Family Medicine Physicians, ENTs and Dentists who do the procedure...but not all do the procedure the same way.
Some practitioners feel there must be a wound visible after clipping for the “release” of the tongue to be “complete”. In our opinion, there are some babies for whom it may be adequate to just clip a few millimeters to help them breastfeed effectively, but it is not enough to help others, so we at MilkWorks usually aim for releasing the tongue completely. Here are “before and immediately after” photos of a baby with a thin mucosa-only frenulum and a very shallow diamond shaped wound:
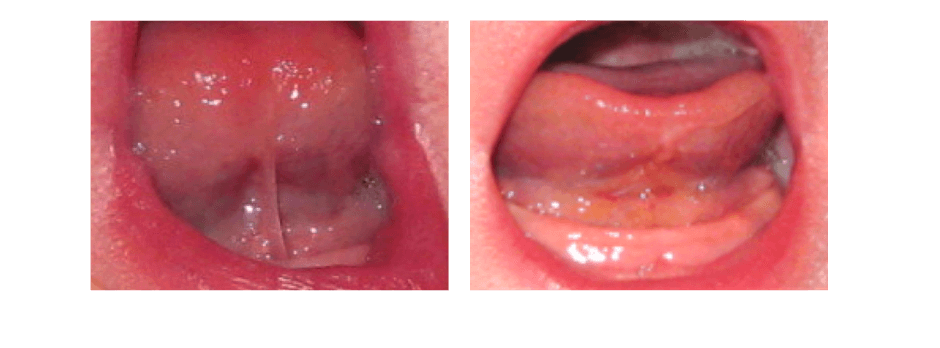
The next day, it will look something like this, as it heals:

These photos result from a frenotomy done with small surgical scissors, which is what we use at MilkWorks. Some people use a laser to divide the tissue instead. There are no studies comparing these 2 methods.
Do I need to stretch the wound after?
Many of the providers who use a laser feel that it is essential to stretch the area multiple times a day for several days after the procedure to keep it from “scarring down”. We have never recommended this, and will wait until there is research proving it is helpful s before we consider recommending this. (We do not know if the healing time/amount of inflammation/chance of scarring is more or less with scissors vs laser) There is one small study looking at stretching vs not with scissors that showed it did not change outcomes: Post Frenotomy Massage for Ankyloglossia in Infants—Does It Improve Breastfeeding and Reduce Recurrence? | SpringerLink
Because of all of this, the most recent “systemic review” (looking at all good studies on this issue) concluded: “Current views of ankyloglossia management leave considerable room for interpretation and variation in practice, leading many mothers to feel frustrated with providers’ conflicting advice and care that is not always aligned with their goals for feeding their infant.” If you are reading this, chances are you can relate to this statement.
Our opinion is that if the baby is not trying to use their tongue effectively and happens to have a frenulum, clipping it is not likely to make any difference, and if they are not trying to lift the tongue along its length to breastfeed well with each suck while nursing, the wound very well may scar down. BUT if the baby IS trying to move their tongue effectively and cannot because it is “tied down”, then freeing it up will allow it to lift with each suck, thus stretching the wound and preventing scarring with each feeding. In our experience, the more normal the suck exam is before clipping (having the baby suck on our finger and seeing what it feels like) the more likely the procedure will be helpful, unless the tongue is tied very close to the tip. When the tie attaches very close to the tip, the suck exam can feel abnormal because movement is so extremely restricted.
What is the optimal age to clip a lingual frenulum?
No one knows. We personally feel the baby deserves to be gaining weight well, not be significantly jaundiced and near due date if born prematurely before we judge their ability to breastfeed.

How does MilkWorks do the procedure?
We wrap the baby in a swaddle blanket and one of the IBCLCs holds the baby’s head still. We use a “grooved director” to hold up the tongue and isolate the frenulum. Then with a very small surgical scissor, we clip the frenulum, hold a 2x2 inch gauze to the site to stop any bleeding, then offer the breast.
IT IS VERY IMPORTANT THAT BABY WANTS TO LATCH AFTER THE PROCEDURE - this usually stops any bleeding very quickly. If baby will NOT suck and is bleeding, we need to continue to hold the gauze in the floor of the mouth. If the baby continues to cry, this can be necessary for 20 mins or more.

How far does MilkWorks clip the frenulum?
We generally clip it far enough to create a small wound at the base of the tongue, but not always. IF a baby is jaundiced, underweight, sleepy we will sometimes just clip the “see through” mucosal portion, so it is much less likely to bleed. If there is a wound, it is usually diamond-shaped, as above. The day after the procedure it will turn white or yellow: and it can take a week or two to be pink again.
What if the bleeding will not stop?
We have a silver nitrate stick we can use to dab onto a spot that will not stop bleeding. This is very rare - each of us has used it once in a combined 40 years.
Important Note: We will not perform a frenotomy if the baby did not receive their Vitamin K shot at birth due to the increased risk of bleeding after leaving our facility.
What is the chance clipping a tongue tie will solve my breastfeeding problems?
We can never promise it will help you – the farther forward the frenulum attaches to the tongue, the more likely it will help. The only problems proven to be improved by clipping are latch difficulty, pain for mom, and difficulty removing milk. There is weak evidence it MAY help spitting up, but this has not been our experience.
What about lip and cheek ties?
Nearly 100% of newborn babies have a “labial frenulum” or lip tie. There is little evidence that clipping or lasering a “labial frenulum” is helpful to breastfeeding. Several studies have looked at breastfeeding babies who had their tongue and lip “ties” “released” at the same time, so the results are difficult to interpret. There is also evidence that the insertion point of a lip tie tends to rise in the mouth as the baby grows older. We do believe that very rarely it is reasonable to divide a very tight labial frenulum that is causing pain directly under the upper lip OR preventing a baby from making a seal and staying latched. We have not been trained to do this procedure and would refer a baby in need to a different provider.
If you STILL want to read more, ENTs (ear nose and throat physicians) published the results of a survey asking questions about tongue, lip and cheek ties: Clinical Consensus Statement: Ankyloglossia in Children - PubMed (nih.gov) Unfortunately, they do not provide references for their statements, but it at least it tells us their opinions. In short, it says the majority of ENTs who responded to the survey DO feel that a tongue-tie can interfere with breastfeeding, BUT a baby should work with a lactation specialist first. There is not clear agreement on lip ties, but there is good agreement that “Buccal ties” (or cheek ties) should not be “released”. (What is a cheek tie? As far as we know right now based on the available research, a “cheek tie” is a normal structure in the mouth that does not cause difficulty with breastfeeding.)
In Summary
The frenotomy providers at MilkWorks have over 40 years combined experience doing this procedure, and will usually NOT do a lingual frenotomy in the following situations:
- Baby did not receive their Vitamin K shot at birth.
- Baby is not breastfeeding. (The only current medical indication for lingual frenotomy is an infant has breastfeeding problems.)
- Baby has not worked with an IBCLC beforehand to see if their problems can be solved with their highly trained breastfeeding help. Research shows that fewer procedures are needed when several disciplines work with the baby first.
- Baby was born premature and has not yet reached their due date.
- Baby is too sleepy to nurse immediately after the procedure. We need them to suckle to stop any bleeding.
- Baby is over 2 months of age. (It is harder to hold an older baby still, and we do not have the sophisticated tools to control bleeding if the older child is crying and refuses to latch)